What Is Genetic Screening? A Practical Guide for Families
TL;DR:
- Genetic screening estimates health risks rather than diagnosing conditions directly, serving as a probabilistic tool. It is particularly useful for pregnant women, individuals with family histories, and those seeking personal risk insights, but requires careful pre- and post-test counseling. Positive results indicate elevated risk, not certainty, emphasizing the importance of follow-up diagnostic testing and informed understanding.
Genetic screening gives families a window into health risks that might otherwise stay hidden until it’s too late to act. But here’s what most people don’t realize: a screening test is not a diagnosis. According to the National Institutes of Health, genetic screening estimates risk rather than confirming a condition. That distinction matters enormously, especially if you’re pregnant, planning a family, or managing a hereditary concern. This guide walks you through exactly what genetic screening is, which types are available, how to read results, and why the conversation with your doctor doesn’t end when results arrive.
Table of Contents
- How genetic screening works: Principles and purposes
- Types of genetic screening: Prenatal and beyond
- Inside cfDNA (NIPT) and carrier screening: How the tests work
- Understanding results, counseling, and limitations
- The real takeaway: What most people get wrong about genetic screening
- Explore more health testing services
- Frequently asked questions
Key Takeaways
| Point | Details |
|---|---|
| Screening shows risk | Genetic screening can estimate your or your child’s risk for certain inherited conditions but cannot confirm a diagnosis. |
| Not all tests are equal | Prenatal screening, cfDNA/NIPT, and carrier screening each serve different purposes and require different follow-up if the result is positive. |
| Counseling is crucial | Expert counseling before and after testing helps you understand what results really mean for your family. |
| Expect follow-up for positives | A positive screening result does not guarantee a condition but does signal the need for further diagnostic testing. |
| Know the limits | All screening tests have technical and biological limitations, making clear communication with your healthcare provider vital. |
How genetic screening works: Principles and purposes
Genetic screening is built around one goal: estimating probability, not delivering certainty. Think of it like a weather forecast. A 70% chance of rain tells you to carry an umbrella. It doesn’t guarantee you’ll get wet. Genetic screening works the same way. It flags elevated risk so that you and your medical team can decide whether further testing makes sense.
This is also what separates screening from diagnostic tests. Understanding the difference between screening versus diagnostic tests is critical for setting realistic expectations. A screening result, even a “positive” one, simply raises a flag. A diagnostic test, like amniocentesis or chorionic villus sampling (CVS), is what actually confirms or rules out a condition. The role of genetic diagnosis in personalized care is to provide clinical certainty where screening can only estimate.
Who benefits most from genetic screening?
- Pregnant women or those planning a pregnancy
- Couples with a family history of inherited conditions
- Individuals in ethnic groups with higher carrier rates for specific disorders
- Anyone who wants to better understand their personal health risks
The screening process typically follows a clear sequence. Before any test is ordered, a healthcare provider reviews your medical and family history and explains what the test can and cannot tell you. This is called pre-test counseling. Then a sample is collected, usually blood or saliva, and sent to a certified lab. Results come back with a risk level, often expressed as a ratio or probability. From there, a post-test counseling session helps you figure out what to do next.
Genetic screening is the use of genetic tests to estimate a person’s or pregnancy’s risk of having (or developing) a genetic condition rather than to definitively diagnose it. — Genomic Screening and Diagnostics: An Introduction, NIH
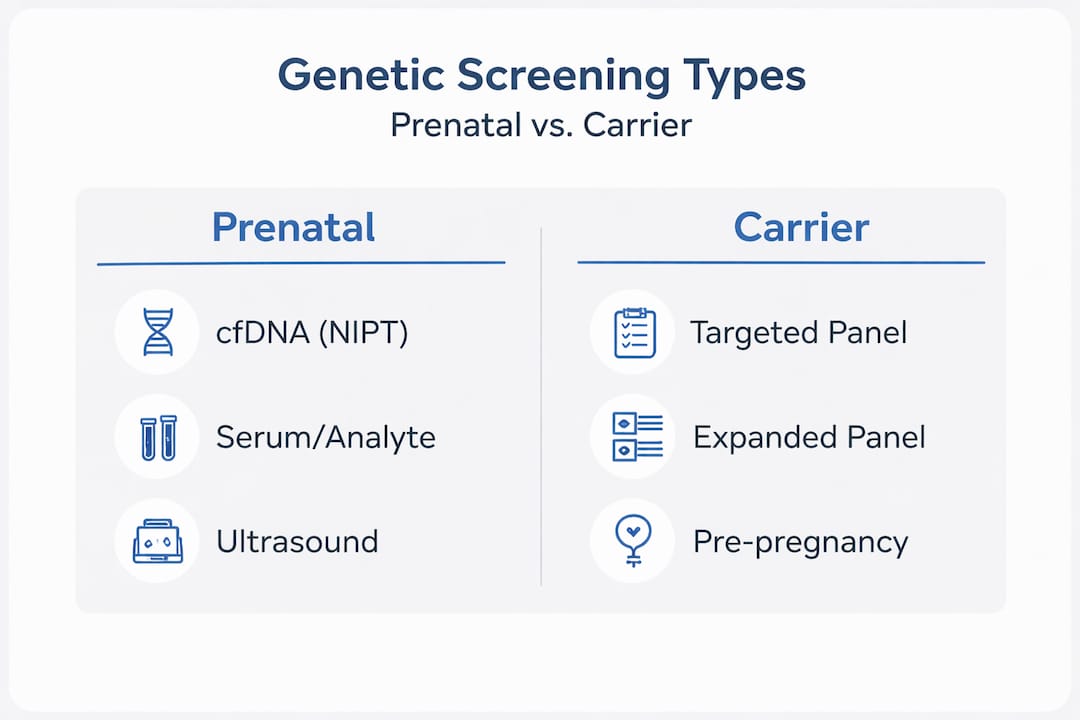
Types of genetic screening: Prenatal and beyond
Now that you understand the purpose of genetic screening, let’s look at the major types and their unique roles.
Prenatal genetic screening has the most established track record. There are three major approaches used during pregnancy, and knowing how each one works helps you and your provider choose the right fit.
| Screening Type | When Used | What It Detects | Key Consideration |
|---|---|---|---|
| Serum/Analyte Screening | 1st or 2nd trimester | Trisomy 21, 18, neural tube defects | Blood markers combined with age risk |
| Nuchal Translucency (NT) | 11 to 14 weeks | Chromosomal abnormalities | Uses ultrasound measurement of fetal neck |
| Cell-Free DNA (cfDNA/NIPT) | 10+ weeks | Trisomies 21, 18, 13; sex chromosomes | Superior detection rates for common trisomies |
Each of these prenatal genetic screening tests serves a specific window in pregnancy and catches different signals. The serum/analyte test measures protein and hormone levels in the mother’s bloodstream. NT screening pairs an ultrasound measurement of the fluid behind the fetal neck with blood markers. cfDNA, also called non-invasive prenatal testing (NIPT), analyzes fragments of fetal DNA floating in the mother’s blood.
Carrier screening: A different purpose entirely
Carrier screening tests adults to find out whether they carry one copy of a gene variant that, combined with another carrier partner, could result in a child with an inherited condition. Cystic fibrosis, sickle cell disease, and spinal muscular atrophy are common examples. Critically, carrier screening is optional. It does not identify every at-risk individual, and counseling about residual risk is always part of the process.
Carrier screening can take two forms. Targeted panels focus on conditions more common in specific ethnic groups, such as Tay-Sachs in Ashkenazi Jewish populations. Expanded carrier screening panels test for hundreds of conditions regardless of ethnicity and are increasingly common.
Other applications worth knowing about
Genetic screening isn’t only for pregnancy. Predictive screening exists for late-onset conditions like hereditary breast and ovarian cancer (BRCA1/BRCA2 variants) and hereditary colorectal cancer syndromes. These tests are typically reserved for individuals with a strong family history or specific clinical criteria, not the general population. Reviewing the types of health screenings that exist can help you understand where genetic screening fits within a broader health plan.
Pro Tip: If you’re unsure whether carrier screening or prenatal screening applies to you, ask your OB-GYN or a genetic counselor before ordering any test. Knowing which panel covers your specific concerns saves time and avoids unnecessary anxiety.
Inside cfDNA (NIPT) and carrier screening: How the tests work
Knowing the types is just the start. Here’s what you need to know about how two of the most important screening methods actually work.
How cfDNA works
During pregnancy, small fragments of the placenta’s DNA circulate in the mother’s bloodstream. These fragments, called cell-free DNA, carry chromosomal information about the developing fetus. A cfDNA test analyzes these fragments to detect whether extra or missing chromosomal material is present. The ACOG practice advisory on cfDNA notes that common lab approaches include sequencing and genotyping methods, and that performance can vary depending on fetal fraction (the percentage of cfDNA that is fetal in origin) and the specific condition being screened.

cfDNA is highly sensitive for trisomy 21 (Down syndrome), trisomy 18 (Edwards syndrome), and trisomy 13 (Patau syndrome). However, its positive predictive value (PPV) varies. PPV is the probability that a positive result is a true positive. In younger patients with lower baseline risk, a positive cfDNA can still often be a false alarm. This is not a flaw in the technology. It’s statistics. That’s exactly why exploring your full DNA testing options before selecting a test is so important.
How carrier screening works
A carrier screening test examines your DNA, typically from saliva or blood, looking for specific variants in genes associated with recessive inherited conditions. If you test positive as a carrier for a condition like cystic fibrosis, you don’t have the condition yourself. The risk only becomes clinically significant when both parents are carriers of the same condition, giving each pregnancy a 25% chance of being affected.
| Carrier Screening Type | Coverage | Best For |
|---|---|---|
| Targeted (ethnicity-based) | 5 to 15 conditions | Known ethnic risk factors |
| Panethnic | ~100 conditions | Couples of mixed or unknown ancestry |
| Expanded panel | 200+ conditions | Broad risk assessment regardless of background |
It’s important to understand that no carrier screening panel catches every possible variant. Residual risk, the small chance of still being a carrier even after a negative result, always exists. Genetic counselors factor this into their discussions with you.
A step-by-step look at the testing process
- Pre-test counseling: Your provider explains what the test covers, what a positive or negative result means, and what follow-up could look like.
- Sample collection: Blood draw or saliva collection, often at a clinic or through a home kit sent to a lab.
- Lab analysis: The sample is processed at a certified laboratory using sequencing or genotyping technology.
- Results delivery: Results typically arrive within 1 to 2 weeks and are reviewed with a provider or genetic counselor.
- Post-result decision making: If results are positive or high-risk, you discuss diagnostic follow-up or family planning options.
Understanding the screening in clinical workflow context helps you see why each step builds on the last. Cutting corners, like skipping counseling or ordering tests without clinical guidance, leads to confusion rather than clarity.
Pro Tip: Ask your lab whether they use sequencing-based or SNP-based cfDNA methods. Sequencing-based methods typically offer higher fetal fraction reliability across all trimesters.
Understanding results, counseling, and limitations
The accuracy and implications of your results can be confusing. Here’s how to make sense of them and where to find support.
Genetic screening results fall into three broad categories:
- Positive or high-risk: The test found markers suggesting an elevated probability of a specific condition. This does not mean your child has the condition. It means further testing is warranted.
- Negative or low-risk: The test found no significant markers. This significantly lowers the probability but does not eliminate all risk.
- Inconclusive or no-call: The test couldn’t produce a clear result, often due to low fetal fraction in cfDNA tests or borderline marker levels.
Clinical guidance from SMFM consistently emphasizes the need for pre-test counseling, genetic counseling after high-risk results, and diagnostic follow-up when indicated. This three-part framework exists because results without context are more harmful than helpful.
Why false positives and negatives happen
Genetic screening limitations are real and documented. False positives can occur due to confined placental mosaicism (where the placenta has chromosomal differences that don’t reflect the fetus), maternal chromosomal variants, or low fetal fraction. False negatives can result from incomplete variant detection or biological variability in marker levels.
Genetic screening has limitations and can produce false positives and false negatives due to factors including technical assay issues, variant interpretation uncertainty, incomplete variant detection, and biological factors such as variable penetrance.
Working with a reliable laboratory that meets rigorous quality standards reduces but does not eliminate these risks.
The role of genetic counseling
The importance of genetic counseling cannot be overstated, especially when results are unexpected. A genetic counselor helps you understand the numerical probability behind your result, explore what diagnostic options exist, and process the emotional weight of an uncertain finding. They also help you think through implications for other family members.
Questions to bring to your appointment:
- What is the detection rate for this specific condition in my age group?
- What is the false-positive rate for this test?
- If results are positive, what diagnostic test would you recommend?
- Does my family history change how we should interpret this result?
- Are there conditions this panel does not cover that I should ask about?
The real takeaway: What most people get wrong about genetic screening
Let’s cut through the myths and see what people often misunderstand about what screening can and cannot do.
The biggest misconception we see is that a negative genetic screening result is the same as a guarantee. Families walk away from a normal cfDNA result feeling completely reassured, and while that relief is understandable, it’s built on an incomplete understanding. Screening reduces uncertainty. It doesn’t eliminate it.
Here’s what that actually means in practice. A negative NIPT result for trisomy 21 dramatically lowers the statistical probability that your child has Down syndrome. But it doesn’t account for every chromosomal abnormality. It doesn’t screen for single-gene disorders unless you’ve added a separate panel. And it doesn’t predict conditions that aren’t yet covered by the test.
On the flip side, families who receive a positive screening result sometimes catastrophize immediately. They assume the worst before diagnostic testing has even been ordered. This creates unnecessary suffering. The data is clear: genetic screening decisions are probabilistic, require follow-up, and carry implications that extend well beyond the test itself.
What we believe strongly, based on how these tests function in the real world, is that informed consent and pre-test counseling aren’t optional extras. They are the mechanism that makes screening results actionable rather than paralyzing. Families who go into testing with realistic expectations make better decisions with their results.
The most empowered position is not the one where you’ve received a clean result. It’s the one where you understand exactly what your result means, what it doesn’t cover, and what your next step is regardless of the outcome. That’s what genetic screening, done right, actually delivers.
Explore more health testing services
After learning how genetic screening fits into your health journey, you might want to explore further services or get help moving forward.
At CountryWideTesting.com, we connect individuals and families with certified laboratory testing that meets the highest quality standards, including CLIA and CAP certification. Whether you’re exploring genetic options, women’s health testing, or other clinical screenings, our lab testing services provide a trusted bridge between questions and answers. Knowing your results come from a verified lab matters as much as the results themselves. Browse our full range of nationwide laboratory tests and find the services that match your family’s health planning needs.
Frequently asked questions
Is genetic screening mandatory during pregnancy?
Genetic screening is optional and offered based on personal and family medical history or patient preference. Carrier screening should be optional, with patients counseled about residual risk and the limits of detection.
Does a positive screening mean my child will have a genetic condition?
No. A positive result means there is an elevated risk, and diagnostic tests confirm conditions where screening only evaluates fetal risk. Diagnostic follow-up is always the next step.
What are the main risks of genetic screening?
The primary risks are emotional and informational: false positives can cause unnecessary worry, while false negatives may provide false reassurance. Screening can produce false results due to technical, biological, and interpretive factors.
How reliable is cfDNA (NIPT) testing?
cfDNA is highly sensitive for common chromosomal conditions, but PPV varies by method and patient risk profile. Diagnostic confirmation is always recommended after a positive cfDNA result.
Why is counseling recommended before and after genetic screening?
Because results are probabilistic and may require follow-up with implications for the whole family, counseling ensures you understand what your result means and what to do next.