Adulteration in Drug Testing: A 2026 Compliance Guide
TL;DR:
- Adulteration in drug testing involves tampering with urine samples to produce false negatives.
- Employers must implement layered controls, including onsite observation and certified laboratory analysis, to detect tampering.
Adulteration in drug testing is the deliberate manipulation of a urine specimen with chemical or physical agents to produce a false-negative result. For HR professionals, employers, and legal consultants, this practice is not a fringe concern. It directly undermines workplace safety programs, exposes organizations to legal liability, and defeats the purpose of any drug-free workplace policy. SAMHSA-regulated testing programs define adulteration as a reportable specimen validity failure, and the 2026 guidelines treat a confirmed adulterated specimen as a refusal to test. Understanding how tampering works, how labs catch it, and how your policies should respond is the foundation of any credible testing program.
What is adulteration in drug testing, and why does it matter?
Adulteration in drug testing refers to the addition of foreign substances to a urine specimen, or the physical substitution of the specimen itself, with the intent to mask drug metabolites. The practice is more common than most employers assume. Donors attempt to beat tests through chemical interference, dilution, or outright substitution with synthetic urine. Each method creates a different detection challenge, and no single countermeasure stops all of them.

The stakes are high for organizations. A false-negative result in a safety-sensitive role can contribute directly to workplace accidents, workers’ compensation claims, and regulatory violations. Legal consultants advising on drug-free workplace programs consistently flag undetected adulteration as one of the most underappreciated sources of compliance risk. The integrity of your testing program depends on understanding what you are up against.
What are the common drug test adulteration methods?
Common chemical adulterants include household bleach, vinegar, salt, glutaraldehyde, nitrites, and oxidants like pyridinium chlorochromate. Each works by chemically degrading drug metabolites in the urine before the immunoassay can detect them. The result is a false-negative reading that looks, on the surface, like a clean specimen.
The most frequently encountered methods fall into three categories:
- Chemical adulteration. Donors add substances directly to the collected specimen. Bleach and vinegar alter the pH. Glutaraldehyde interferes with enzyme-based immunoassays. Nitrites and pyridinium chlorochromate oxidize THC metabolites specifically, which is why they became popular among cannabis users.
- Dilution. Donors drink large volumes of water before collection to reduce metabolite concentration below detection thresholds. Internal dilution leaves metabolic and biomarker ratio signatures beyond creatinine, but basic dip card tests often miss these patterns.
- Substitution. Donors replace their urine entirely with synthetic urine or another person’s clean specimen. Synthetic urine products are commercially available and formulated to mimic normal creatinine and pH values, making them harder to catch without temperature checks and advanced validity testing.
Pro Tip: Require temperature verification immediately at collection. A specimen outside the 90°F to 100°F range at the time of collection is a strong indicator of substitution and should trigger immediate documentation.
Novel psychoactive substances and newly developed adulterants create detection challenges that require ongoing lab protocol updates. Relying solely on standard protocols leaves employers vulnerable to sophisticated tampering. The adulterant market evolves in direct response to detection advances, which means your program must too.
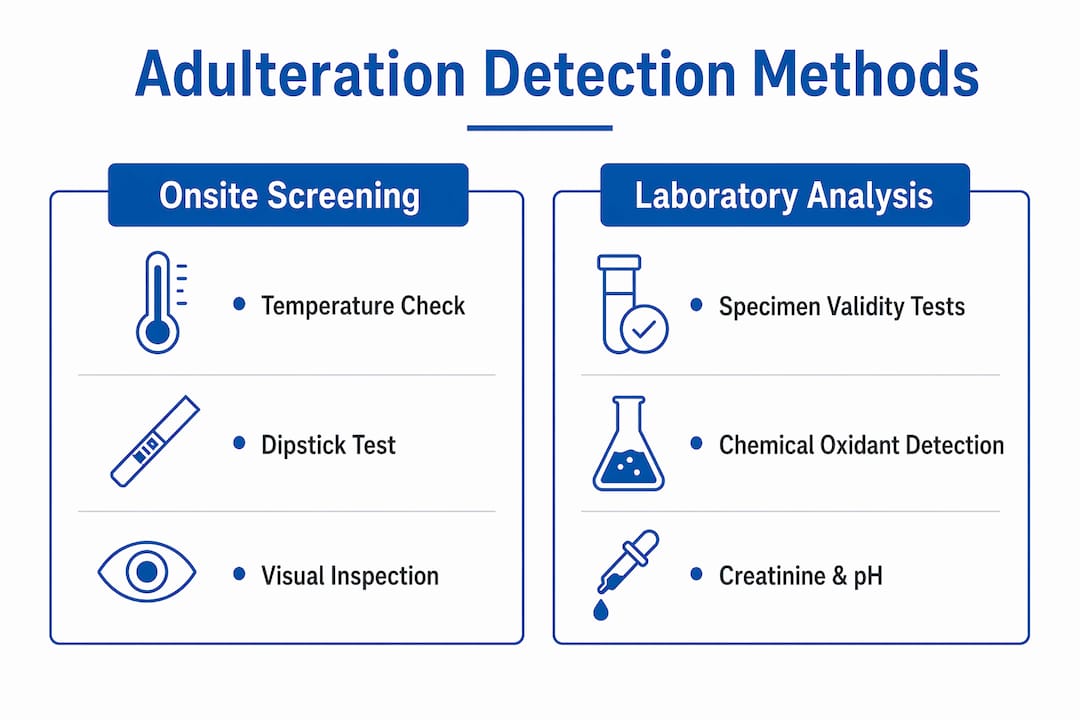
How do laboratories detect adulteration and maintain specimen integrity?
Laboratory detection of adulteration relies on specimen validity testing, a structured set of measurements applied to every urine specimen before immunoassay screening begins. Specimen validity tests include assessments of urine temperature, pH, creatinine, and specific gravity to identify adulterated samples. Values outside standard reference ranges raise tampering suspicions and trigger further investigation.
The standard validity testing sequence follows this order:
- Temperature check. Performed at the collection site within four minutes of voiding. A reading outside the 90°F to 100°F range flags possible substitution.
- pH measurement. Normal urine pH falls between 4.5 and 8.5. Readings outside this range indicate chemical adulteration, often from bleach or acid-based adulterants.
- Creatinine and specific gravity. Low creatinine below 2 mg/dL combined with low specific gravity below 1.001 signals substitution with water or synthetic urine. Dilute specimens show creatinine between 2 and 20 mg/dL.
- Specialized chemical assays. Sophisticated lab assays detect compounds such as glutaraldehyde and pyridinium chlorochromate, often missed by basic dipstick tests. These oxidizing agents cause drug metabolite chemical degradation but are identifiable via specialized tests.
- Confirmatory instrumented analysis. Gas chromatography-mass spectrometry (GC-MS) and liquid chromatography-mass spectrometry (LC-MS) confirm the presence of specific adulterant compounds at the molecular level.
The gap between basic onsite testing and full laboratory analysis is significant. A dipstick test at the collection site checks pH and creatinine. A SAMHSA-certified laboratory runs the full validity panel and applies instrumented confirmation. That difference is where most sophisticated adulteration attempts are caught or missed.
Pro Tip: Always send specimens to a CLIA-certified or CAP-accredited laboratory for confirmation. Onsite strips are a useful first screen, but they are not a substitute for instrumented laboratory analysis.
| Detection method | What it catches | Limitation |
|---|---|---|
| Temperature strip | Substitution | Must be checked within 4 minutes |
| pH dipstick | Bleach, acid adulterants | Misses glutaraldehyde and nitrites |
| Creatinine/specific gravity | Dilution, substitution | Does not detect chemical oxidants |
| Specialized chemical assay | Glutaraldehyde, chromium compounds | Requires certified laboratory |
| GC-MS / LC-MS confirmation | Specific adulterant compounds | Cost and turnaround time |
What regulatory standards govern adulteration detection?
SAMHSA 2026 guidelines mandate the use of Medical Review Officers to review all non-negative and adulterated samples, ensuring legal and medical verification. An MRO is a licensed physician trained to interpret drug test results in the context of medical history and prescription use. No employer covered by federal drug-free workplace requirements should be reporting results directly from the laboratory without MRO review.
The regulatory framework creates specific obligations for employers:
- Adulterated specimens are treated as refusals to test. Under SAMHSA standards, adulterated specimens trigger predefined consequences and documentation requirements. This means your policy must define what happens when a specimen is reported as adulterated, not just when a test is positive.
- MRO review is mandatory for non-negative results. The MRO contacts the donor directly to determine whether a legitimate medical explanation exists before reporting the result to the employer. Understanding the MRO’s role in this process is critical for HR teams managing federal contractor or DOT-regulated programs.
- Records must be confidential. Access to drug test results must be restricted to individuals with a need to know. Broad internal sharing of test results creates legal exposure under ADA and state privacy laws.
- Policies must define refusal consequences explicitly. Vague policies create litigation risk. A donor who refuses to provide a specimen, or whose specimen is reported as adulterated, must face the same documented consequences as a positive result.
Employers outside federally mandated programs still benefit from aligning with SAMHSA standards. Courts and arbitrators consistently treat SAMHSA-compliant procedures as the benchmark for defensible drug testing. Deviation from those standards weakens your position in any challenge.
What practical strategies can employers use to prevent drug test cheating?
Preventing adulteration requires a layered approach. No single control stops all tampering methods. The combination of collection-site controls, onsite screening, laboratory confirmation, and written policy creates a program that is genuinely difficult to defeat.
- Use direct observation when authorized. Visual observation during collection reduces tampering risks but does not eliminate adulteration. Direct observation is permitted under federal guidelines for return-to-duty and follow-up testing, and for collections where there is reason to believe tampering occurred.
- Deploy onsite adulteration strips. Adulteration test strips provide quick onsite screening for specimen validity, complementing laboratory confirmation. Strips detect abnormalities in pH, creatinine, and the presence of adulterants within minutes. They are not a final answer, but they flag suspicious specimens before the chain of custody is broken.
- Train collection site staff. Supervisors and collection staff should know the signs of drug sample tampering: unusual specimen color, temperature outside range, strong chemical odor, or a donor who requests an unusually long time in the restroom. Documented observations support defensible decisions if a result is challenged.
- Write explicit policies. Clear written policies that define refusal to test, consequences of adulteration, and documented supervisor observations reduce legal risk and support defensible decisions. Policies should be reviewed annually to reflect changes in SAMHSA guidelines and state law.
- Review your program annually. The most common drug tests for employment have changed as the drug landscape shifts. Programs built around five-panel urine tests in 2018 may not detect the substances most prevalent in your workforce today.
Pro Tip: Integrate a guide to drug test adulteration into your new-hire supervisor training. Supervisors who understand what adulteration looks like are far more effective at flagging suspicious collections than those who only know how to fill out paperwork.
Workplace drug testing programs must evolve continuously to detect emerging adulterants and novel substances, integrating technology and policy. A program that was defensible three years ago may have gaps today.
The uncomfortable truth about adulteration detection
The drug testing industry talks a great deal about detection technology, and the technology genuinely has improved. But the most common failure point I see is not the laboratory. It is the gap between what a policy says and what actually happens at the collection site.
Employers invest in certified labs and MRO partnerships, then undermine the whole system by using collection sites that skip temperature checks, allow donors unsupervised access to water sources, or fail to document unusual observations. A sophisticated adulterant caught by a $400 laboratory assay means nothing if the specimen was compromised before it left the bathroom.
Clinical experts emphasize that a combination of observation, laboratory testing, and clear policies provides the best defense against adulteration. That combination only works when all three elements are actually implemented, not just described in a policy document.
The other thing worth saying plainly: donor rights matter. Treating every donor as a suspected cheat creates a hostile environment and invites legal challenges. The goal is a program that is rigorous enough to catch actual tampering while treating honest donors with professional respect. That balance is achievable, but it requires deliberate design, not just a checklist.
— Alan
Countrywidetesting’s lab services for employer drug testing programs
Employers who need reliable adulteration detection backed by certified laboratory science can access those services directly through Countrywidetesting.
Countrywidetesting partners with SAMHSA-compliant, CLIA-certified, and CAP-accredited laboratories to deliver lab screening services that include full specimen validity testing and specialized adulterant detection assays. MRO review is integrated into the confirmation workflow, so HR teams receive results that are already legally defensible. Whether you are building a new workplace testing program or updating an existing one to meet 2026 standards, Countrywidetesting provides the laboratory infrastructure and compliance support to do it right.
FAQ
What does an adulterated drug test result mean?
An adulterated result means the specimen contains a foreign substance that interferes with testing. Under SAMHSA standards, it is treated as a refusal to test and triggers the same consequences as a positive result.
What are the most common adulterants used in urine drug tests?
The most common adulterants are bleach, vinegar, salt, glutaraldehyde, nitrites, and pyridinium chlorochromate. Each degrades drug metabolites or disrupts the immunoassay process to produce a false-negative reading.
Can a basic dipstick test detect all adulterants?
No. Basic dipstick tests check pH and creatinine but miss sophisticated oxidizing agents like glutaraldehyde and chromium compounds. Instrumented laboratory assays are required to detect those substances reliably.
What role does an MRO play in adulterated specimens?
A Medical Review Officer reviews all non-negative and adulterated results, contacts the donor for a medical explanation, and reports a final verified result to the employer. This step is mandatory under SAMHSA-regulated programs.
How should employers document an adulterated specimen?
Employers should record the collection site observations, the laboratory validity report, and the MRO’s final determination. Written policies must specify the consequences, and all records must be kept confidential with restricted access.
Key takeaways
Adulteration detection requires layered controls: collection-site procedures, onsite screening, certified laboratory analysis, and written policies that treat adulterated specimens as refusals to test.
| Point | Details |
|---|---|
| Adulteration defined | Deliberate tampering with urine specimens to produce false-negative results, classified as a refusal to test under SAMHSA standards. |
| Common adulterant types | Bleach, glutaraldehyde, nitrites, and pyridinium chlorochromate are the most frequently detected chemical adulterants. |
| Laboratory detection is essential | Onsite strips screen for basic anomalies; only certified lab assays reliably detect sophisticated oxidizing agents. |
| MRO review is mandatory | All non-negative and adulterated specimens must be reviewed by a Medical Review Officer before results reach the employer. |
| Policy and training close the gap | Clear written policies and trained collection staff are as critical as laboratory technology in preventing successful adulteration. |