Why Instant Drug Tests Fail: Causes and Limitations
TL;DR:
- Instant drug tests produce only presumptive results due to cross-reactivity, which can lead to false positives or negatives. Confirmatory lab tests like GC-MS are mandatory for definitive results, especially in safety-sensitive roles. Procedural errors and specimen issues can invalidate results, emphasizing the need for proper collection, handling, and confirmation protocols.
Instant drug tests are defined as immunoassay-based screening tools that detect molecular shapes rather than exact chemical identities, which is the root cause of why instant drug tests fail to deliver definitive results. These devices produce presumptive findings only. They cannot confirm the presence of a specific drug with the certainty required for employment decisions, legal proceedings, or safety-sensitive roles. Colorimetric field drug tests show error rates between 15% and 38%, contributing to roughly 30,000 wrongful arrests annually in the U.S. That scale of error makes understanding these limitations not just useful but necessary for anyone relying on rapid test results.
Why instant drug tests fail: the chemistry behind false results
Immunoassay technology is the foundation of every rapid drug test, and its core mechanism is also its greatest weakness. Antibodies bind to molecular shapes, not unique chemical fingerprints. That means any substance with a similar molecular structure can trigger a positive result, even if no illicit drug is present.

This phenomenon is called cross-reactivity, and no manufacturing improvement can eliminate it. Every immunoassay kit ships with a cross-reactivity table listing known interferences. That table exists because the problem is structural, not accidental.
Common substances that trigger false positives include:
- Ibuprofen and naproxen (NSAIDs): can register as marijuana metabolites on some panels
- Pseudoephedrine (found in cold medicines like Sudafed): may trigger amphetamine positives
- Quinolone antibiotics: linked to false opiate readings
- Poppy seeds: contain trace morphine that can exceed opiate detection thresholds
- Soap and chocolate: generic color-change chemistry in colorimetric field tests has flagged both as controlled substances
False negatives are equally common. When a drug concentration falls below the test’s cutoff threshold, the result reads negative even if the substance is present. Synthetic cannabinoids and designer drugs often escape detection entirely because their molecular structures differ enough from the antibody targets.
The difference between a screening test and a confirmatory test matters here. Screening tests cast a wide net to catch probable positives quickly. Confirmatory methods like gas chromatography-mass spectrometry (GC-MS) identify exact chemical structures and concentrations. GC-MS does not guess at molecular shape. It reads the compound directly.
Pro Tip: If you receive a positive result on a rapid test, request GC-MS confirmation before any employment or legal action is taken. A presumptive positive is not a proven positive.
What procedural errors cause instant drug test failures?
Even a chemically sound test can produce an invalid result when the collection or handling process breaks down. Procedural failures are a leading cause of drug testing errors, and many of them are entirely preventable.
Nine specific procedural errors are defined under 49 CFR Part 40 as “fatal flaws.” These errors automatically cancel a test, meaning the result cannot be used and the test must be repeated. Fatal flaws include missing or incomplete Custody and Control Forms (CCFs), broken specimen seals, and mismatched specimen IDs.
The most common procedural problems fall into four categories:
- Expired or improperly stored devices. Rapid test kits degrade over time. An expired device may produce a false negative or an invalid reading. Storage above recommended temperature ranges accelerates reagent breakdown.
- Specimen integrity failures. Dilute urine, caused by excessive hydration before the test, pushes drug concentrations below detection thresholds. Contaminated samples, whether from cleaning products or adulterants added to the specimen, interfere with antibody reactions.
- Temperature and timing errors. Urine specimens must fall within a specific temperature range (90°F to 100°F) immediately after collection. A specimen outside that range signals possible substitution or tampering and must be flagged.
- Chain of custody breakdowns. Missing Custody and Control Forms or broken seals invalidate results under federal rules. Without a documented chain of custody, no result is legally defensible.
An invalid result is not the same as a failed test. An invalid result means the lab could not produce a reliable outcome due to specimen issues or interference. It requires retesting or Medical Review Officer (MRO) review, not automatic disqualification. Employers and individuals who treat an invalid result as a positive make a serious procedural error.
Pro Tip: Employers should audit their collection site procedures at least annually. A single chain of custody gap can void an otherwise valid result and expose the organization to legal liability.
How do instant tests compare to lab-based confirmation testing?
Instant tests and laboratory confirmation testing serve different purposes. Treating them as equivalent is the most consequential misunderstanding in drug testing practice.
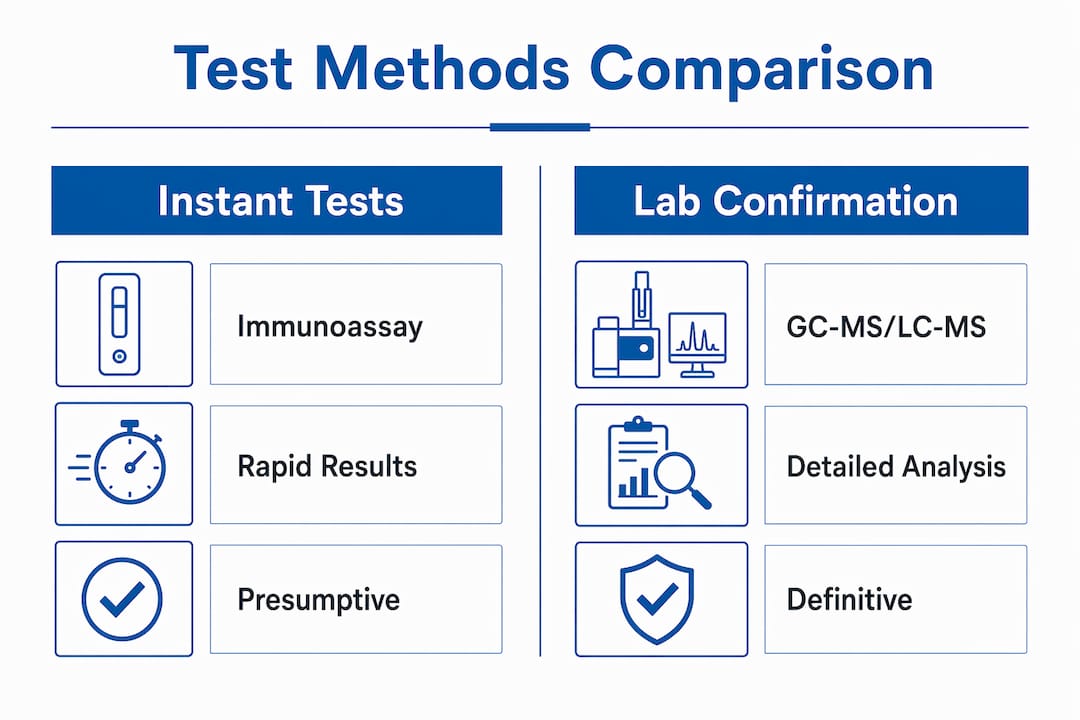
The table below outlines the key differences:
| Feature | Instant (immunoassay) test | Lab confirmation (GC-MS/LC-MS) |
|---|---|---|
| Detection method | Molecular shape recognition | Exact chemical structure identification |
| Result type | Presumptive (positive/negative) | Definitive (confirmed or not confirmed) |
| Turnaround time | Minutes | 24–72 hours |
| Cross-reactivity risk | High | Negligible |
| Legal admissibility | Limited without confirmation | Accepted in legal and regulatory proceedings |
| Required for DOT roles | Screening only | Mandatory for all positives |
Under 49 CFR Part 40, the Department of Transportation requires that all presumptive positives in safety-sensitive roles be confirmed by a certified laboratory before any adverse action is taken. This rule exists precisely because instant tests produce too many inaccurate results to stand alone. Employers in transportation, aviation, and federal contracting who skip this step face fines and legal exposure.
Lab methods like GC-MS and liquid chromatography-mass spectrometry (LC-MS) do not rely on antibody binding. They separate compounds chemically and measure their exact mass-to-charge ratios. A GC-MS result identifying methamphetamine is not a guess. It is a chemical fact.
Experts at ARUP Consult state that instant positive results are starting points only and require further investigation before any consequential decision is made. That guidance applies equally to employers, law enforcement, and healthcare providers. The comparison between instant and lab testing is not about speed versus accuracy as a preference. It is about using each tool for its intended purpose.
Electronic testing devices using laser or infrared technology offer better specificity than colorimetric tests. They reduce cross-reactivity errors without requiring full lab infrastructure. These devices represent a meaningful improvement for field use, though they still do not replace certified laboratory confirmation for legal or employment purposes.
How to reduce errors and handle instant test results responsibly
Rapid test results require a structured response, not an immediate conclusion. Both individuals and employers can take concrete steps to reduce the risk of acting on a flawed result.
- Disclose all medications and supplements before testing. Medical Review Officers review prescription drug use to determine whether a positive result has a legitimate medical explanation. Failing to disclose creates unnecessary complications.
- Treat every presumptive positive as unconfirmed. Instant tests serve as preliminary screening and are not diagnostic tools. A positive result on a rapid test does not prove drug use.
- Request lab confirmation for any positive result. GC-MS or LC-MS confirmation is the only method that produces a legally defensible finding. Employers in regulated industries are required to follow this step under federal rules.
- Maintain strict chain of custody from collection to result. Document every transfer of the specimen. Use tamper-evident seals. Verify that CCFs are complete before the specimen leaves the collection site.
- Understand what an invalid result means. An invalid result is a procedural outcome, not a positive finding. It requires retesting under MRO guidance, not disciplinary action.
- Consider electronic testing devices for field screening. Laser and infrared devices reduce false positives compared to colorimetric tests. For employers running high-volume screening programs, the upgrade pays for itself in avoided disputes.
Employers setting up DOT-compliant drug testing programs should build confirmation testing into their standard operating procedures from day one. Retrofitting a process after a wrongful termination dispute is far more costly than building it correctly at the start. For post-accident drug testing, the stakes are even higher because results may enter legal proceedings.
Key Takeaways
Instant drug tests produce presumptive results only, and every positive finding requires GC-MS or LC-MS lab confirmation before any employment, legal, or safety decision is made.
| Point | Details |
|---|---|
| Chemistry causes false positives | Immunoassay antibodies bind molecular shapes, so common medications and foods can trigger incorrect positives. |
| Procedural errors void results | Fatal flaws like missing CCFs or broken seals automatically cancel tests under 49 CFR Part 40. |
| Lab confirmation is mandatory | DOT and other federal regulations require certified lab confirmation of all presumptive positives in safety-sensitive roles. |
| Invalid results need retesting | An invalid result is not a positive finding. It requires MRO review and specimen retesting. |
| Disclosure protects individuals | Reporting all medications to the MRO before testing prevents legitimate prescriptions from being misread as violations. |
The part nobody tells you about rapid test results
I have spent years watching organizations make the same mistake: they treat a rapid test result as a verdict. A positive strip on a urine cup becomes grounds for termination before anyone asks whether the person takes ibuprofen daily or drinks poppy seed tea. That is not a testing failure. That is a policy failure.
The science here is not ambiguous. False-positive rates reach as high as 91% in certain correctional settings. That number should stop anyone cold. It means that in some environments, the majority of positive rapid test results are wrong. Acting on those results without confirmation is not just unfair. It is statistically indefensible.
What frustrates me most is that the solution is not complicated. GC-MS confirmation exists. MRO review exists. Chain of custody protocols exist. The current drug testing trends show that more agencies are adopting cite-and-release policies that delay consequences until lab results return. Law enforcement increasingly recognizes that speed without accuracy produces injustice, not safety.
My advice to any employer or individual navigating a positive rapid test result: slow down. The test told you something might be present. It did not tell you what, how much, or whether it matters legally. Get the confirmation. Protect yourself and the person being tested.
— Alan
Accurate drug testing starts with the right tools
Rapid screening has its place, but it cannot be the last word on a drug test result. Countrywidetesting provides lab-based drug testing services certified under SAMHSA, ISO, CLIA, and CAP standards, giving individuals and employers results that hold up legally and clinically.
For situations where a presumptive positive needs confirmation, Countrywidetesting offers the Phamatech urine lab confirmation mail-in test, a straightforward option for getting a certified result without visiting a clinic. Employers managing regulated programs can also access the SAMHSA seven mail-in confirmation test for federally compliant follow-up testing. Every result processed through Countrywidetesting’s lab partners meets the confirmation standards required by federal regulations.
FAQ
Why do instant drug tests produce false positives?
Instant drug tests use immunoassay chemistry that detects molecular shapes rather than specific drug compounds. Common substances like ibuprofen, cold medicine, and certain foods share molecular similarities with target drugs, triggering false positives through cross-reactivity.
Is an invalid drug test result the same as a positive?
An invalid result is not a positive finding. It means the specimen could not be reliably analyzed due to dilution, contamination, or interference, and it requires retesting or Medical Review Officer review before any conclusion is drawn.
What confirmation method is required after a rapid test positive?
Gas chromatography-mass spectrometry (GC-MS) or liquid chromatography-mass spectrometry (LC-MS) is the standard confirmation method. Under 49 CFR Part 40, all presumptive positives in safety-sensitive roles must be confirmed by a certified laboratory before any adverse action is taken.
What are fatal flaws in drug testing?
Fatal flaws are specific procedural errors, defined under 49 CFR Part 40, that automatically cancel a drug test result. Examples include missing Custody and Control Forms, broken specimen seals, and mismatched specimen identification numbers.
Can drinking water before a drug test cause a false negative?
Excessive hydration before a test dilutes urine, pushing drug concentrations below the test’s detection threshold. A dilute specimen may produce a negative result even when a drug is present, and it often triggers a request for a repeat collection.